
Why Phase One Treatment Can Be Important For Your Child

By Dr. M. Constance Greeley
Last issue, we covered some of the important reasons for early orthodontic treatment. Those reasons included habits, sleep disturbed breathing and apnea. (Please see the 4th quarter 2018 issue of The County Women’s Journal for details.)
There are several other conditions that warrant Phase One Treatment which I will address in this article.
Ectopic Eruption:
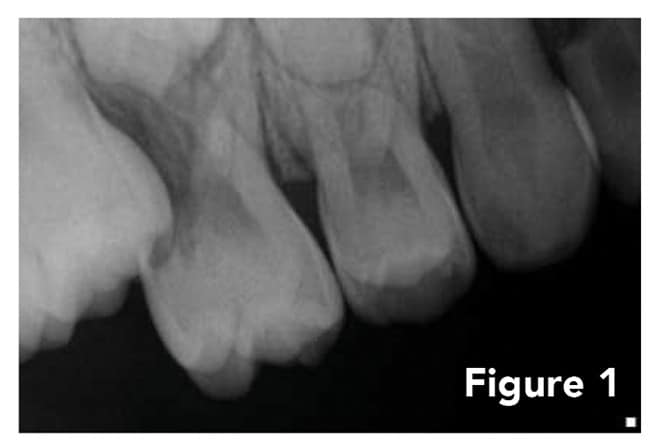
Most of the time, children are referred to orthodontists because their dental crowding becomes obvious as permanent teeth begin to come in (we use the term “erupt”). This is a good prompt because it alerts us to impending problems that are not always obvious until a thorough exam is done. For example, some permanent molars (often called “6 year” molars) can get caught behind the baby molars. It is referred to as “ectopic” as in “out of place.” These permanent molars can resorb (i.e., dissolve) the roots of the baby molars causing the baby molars to either come out too early, become decayed, and/or cause pain for the patient. Early loss of the baby molar then diminishes space for the permanent bicuspid that needs to eventually come into that spot. Early treatment addresses this problem, saving the patient from more complex and costly treatment later. Molars are the most common ectopic eruptors but there are several other teeth that can “get lost” trying to come in. (Figure 1)
Impacted Teeth:
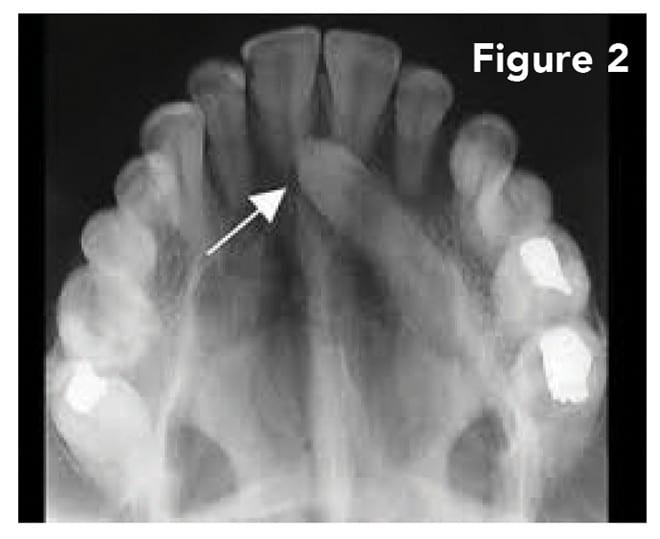
The inability of teeth to come into the mouth is known as “impaction.” The teeth most likely to be impacted (besides “wisdom teeth”) are the upper permanent canines (“eye teeth”). These teeth are important corner-stones of the arch. Impaction tendencies can run in the family, so discussing family dental history helps alert us to possible problems. Impacted canines can create serious issues including the possible melting away (resorbing) of the roots of adjacent front permanent teeth. If ignored, the patient may need extensive orthodontic treatment that can also require surgical uncovering of the impacted teeth or possibly extraction resulting in other challenges that are both functional and esthetic. Instead, these conditions can be alleviated by early upper arch expansion, an easy procedure for the child, and sometimes early removal of the baby canines (also not traumatic) to help redirect the permanent teeth. Early identification and treatment of these issues save the patient from extensive treatment later and simplifies Phase Two orthodontic treatment in the adolescent. (Figure 2)
Extra Teeth:
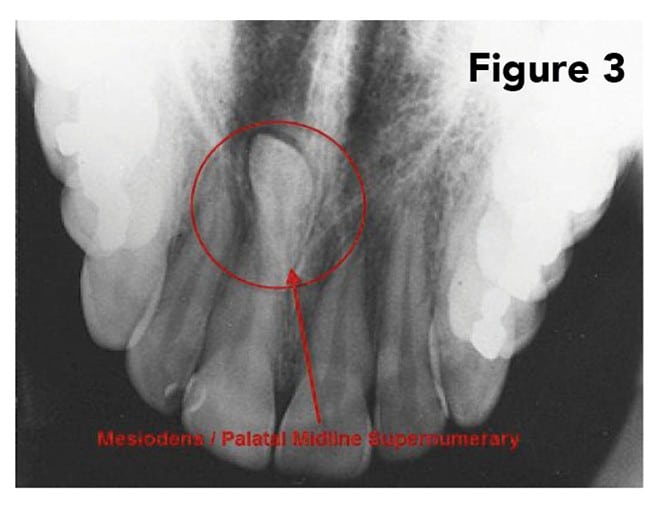
Another common occurrence is the development of extra teeth. We often refer to them as “supernumerary” teeth. That’s a big word for small teeth that can cause big issues. The most common place for extra teeth to develop is between the upper front teeth (often called a “mesiodens”). These teeth can be tiny pearl-like entities or fully developed with roots and sometime be upside down! If these teeth develop in close proximity to the upper permanent incisors, they can interfere with the eruption of these front teeth. So, while your child’s peers are getting their upper front teeth, your child may still be waiting for theirs. Good idea to check out if the wait is “normal” for your child or if there is an obstruction such as an extra tooth causing the delay. Extra teeth can develop anywhere. Sometimes they can be ignored and just followed periodically. Sometimes they require removal. (Figure 3)
A base-line panoramic x-ray of your child’s mouth, low in radiation exposure, can help uncover all these conditions and is well worth the trip to the orthodontist. Again, an ounce of prevention . . . as they say!
My favorite assessment to make is “All looks good for now. Let’s follow up in 6 months or so.”
About
Dr. Connie Greeley did her undergraduate work majoring in Pharmacy at Temple University. After graduating, she remained a student on campus at the School of Dentistry where she received her Doctor of Dental Surgery degree. She was an honor student in college and dental school. She earned her certification in Pediatric Dentistry at the University of Maryland and then returned to Temple University for her certification in Orthodontics.
Dr. Greeley is board-certified by the American Board of Orthodontics. She serves on the Cleft Palate Team at A.I. DuPont Hospital for Children and is on the volunteer teaching staff at Christiana Care Wilmington Hospital Department of Dentistry. Dr. Greeley is past-president of the Delaware State Dental Society, the Middle Atlantic Society of Orthodontists, and the Greater Philadelphia Society of Orthodontics. She is a member of the American Dental Association and the American Association of Orthodontists.
transform your life with a beautiful smile at:
Greeley Orthodontics, PA
400 Old Forge Lane, Suite 406
Kennett Square, PA 19348
484-346-7846
![]()

{kind=link}